Article Text

Abstract
Objective Quality improvement (QI) practices and scholarship are increasingly concerned with environmental sustainability given the negative health outcomes caused by the ecological crisis, as well as the environmental impacts of healthcare delivery itself. A core component of QI activities is measuring change. How sustainability metrics have been used in QI is unclear. We conducted a scoping review of metrics used in published sustainability-focused QI initiatives.
Data sources MEDLINE, EMBASE, CINAHL and Scopus from 2000 to 2023.
Eligibility criteria Published healthcare QI initiatives intended to address environmental sustainability with at least one quantitative sustainability metric.
Data analysis Publication, study, measurement and QI intervention characteristics were charted from included studies. Data items were synthesised and presented narratively as well as quantitatively.
Results We screened 6294 studies and included 90 full-text publications. The studies were published from 2000 to 2023, with the majority (61%, 55/90) published since 2020. Publications originated from a wide range of clinical disciplines with most QI projects situated in the inpatient setting (78%, 70/90). Environmental sustainability metrics were subcategorised into activity data and environmental impact indicators. Some papers included more than one category of activity data, with the most common being cost (88%, 79/90), hospital waste (52%, 47/90), anaesthetic gases (49%, 44/90), disposable use (24%, 22/90) and distance travelled (14%, 13/90). Fewer publications included environmental impact indicators, with global warming potential dominating this category (53%, 48/90).
Discussion There is a need to align QI efforts with environmental sustainability. However, there is limited guidance specific to healthcare QI on how to measure environmental impacts of these efforts. This review illuminates that sustainability-focused QI efforts to date have used a relatively narrow set of sustainability metrics. QI scholars and practitioners can benefit from further education, measurement frameworks and guidelines to effectively incorporate environmental sustainability metrics into QI efforts.
- Quality improvement
- Healthcare quality improvement
- Crisis management
- Quality measurement
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
There is a growing body of literature on quality improvement (QI) initiatives aiming to address environmental sustainability.
WHAT THIS STUDY ADDS
QI practitioners have predominantly used activity data rather than measures of environmental impact for sustainability metrics. Those studies reporting measures of environmental impact rarely reported impacts other than global warming potential.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
To ensure QI initiatives are truly impacting environmental sustainability, future QI and clinical innovation work should take a more holistic view of sustainability by considering as broad a set of environmental impact categories as is applicable and feasible. This view ought to be embedded in QI guidelines, institutional policy and strategic planning.
Introduction
Growing attention to the environmental impacts of healthcare delivery, alongside mounting health human resource constraints and rising healthcare costs, has elevated sustainability as a key domain of healthcare quality.1 The healthcare sector constitutes approximately 4.4% of total global carbon emissions through direct care delivery (eg, use of anaesthetic gases with high global warming potential (GWP)), the need for electricity (which may derive from carbon-intensive energy sources) and through the supply chain (eg, manufacturing of pharmaceuticals).2 Further, healthcare delivery, especially in resource-intensive hospital settings, generates considerable waste, including of single-use plastic and other disposables such as laboratory and surgical supplies.3
The healthcare system must also grapple with the human health harms and societal instability, resulting from the climate crisis and large-scale climate change-related events such as heatwaves and flooding.4 For example, air pollution and poor air quality generated by fossil fuel combustion are estimated to drive an annual excess 8.34 million deaths globally through cardiometabolic and respiratory diseases.5 6 Healthcare systems and providers aim to improve health; therefore, care delivery must minimise emissions to reduce environmental and health harms.
Efforts to reduce emissions include initiatives to eliminate unnecessary care, make care more efficient and address the underlying social determinants of health to reduce demand for healthcare services. Recognising the alignment of quality and environmental sustainability, an increasing number of healthcare providers and organisations have sought to use quality improvement (QI) to mitigate the environmental impacts of healthcare.7 Despite the emerging consensus that the healthcare sector must undergo a sustainability transformation and that QI has much to offer in this regard, little is known about how QI practitioners have mobilised existing approaches to tackle environmental concerns.
QI relies on robust data collection around quality measures (including outcome, process and balancing measures) to determine whether an intervention is having the desired effect.8 These measures are intended to assess improvements towards QI goals. Yet the desired effect in terms of environmental impact is not within the realm of traditional QI measures and data holdings. QI practitioners thus face the difficult task of selecting among environmental sustainability metrics. These environmental sustainability metrics describe a range of environmental impacts including but not limited to GWP and are commonplace in the environmental foot printing literature.9 However, QI practitioners may have little familiarity with the range of environmental impacts—and thus metrics—associated with healthcare activities.
The lack of standardisation in defining and measuring environmentally sustainable healthcare has been noted elsewhere; when it comes to measurement, there is variability in terms of both what is being measured and how.10 Furthermore, measurement is critical to ensure QI does not have unintended consequences. To illustrate, efforts to substitute total intravenous anaesthesia (TIVA) for inhaled anaesthetic gases with high GWP may mitigate carbon emissions. However, TIVA anaesthetic has demonstrated toxicity when disposed of incorrectly with deleterious effects on aquatic life and other living organisms.11 It is therefore imperative that greater sophistication is pursued in the measurement of environmental impacts in QI.
The aim of this scoping review is to describe the range of measurement approaches and measures used in environmental sustainability-focused QI efforts. This will serve as a starting point for developing guidance on the use of such measures in clinical and scholarly work related to QI projects focused on environmental sustainability.
Methods
Protocol and registration
The scoping review was designed in keeping with the Arksey and O’Malley framework, which identifies five required steps for conducting a scoping review and reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for scoping reviews (online supplemental table 1).12 13 The protocol was published previously and articulated the first step of the scoping review, identifying a research question or primary aim, which is to better understand how existing QI efforts to address environmental sustainability in healthcare have attempted to identify and measure ecological impacts.14 The scoping review approach was chosen because the aim is to map the character and extent of a rapidly growing and heterogeneous body of literature, and not to arrive at a precise effect estimate.15
Supplemental material
Identifying relevant studies
We designed a comprehensive search strategy in collaboration with experienced information specialists and a QI research synthesis expert. The terms capturing QI and clinical innovation efforts included variations on key words for QI (eg, clinical innovation) and sustainability (eg, waste, carbon, environment). The healthcare setting was captured using variations on the term ‘healthcare’ (eg, hospital, operating room). The strategy was validated through the retrieval of several key studies, determined a priori to meet inclusion criteria. The full MEDLINE search strategy is detailed in online supplemental appendix 1. We limited our search to published literature in peer-reviewed literature.
MEDLINE, EMBASE, CINAHL and Scopus were searched using database-specific search strategies for peer-reviewed literature published between 2000 and 2023 in the English language. The MeSH (Medical Subject Headings) terms selected for the search in MEDLINE were adapted to corresponding headings in each database. We chose to limit our results to those published after 2000 because the seminal report that popularised the quality and patient safety movement, To Err is Human, was published in this year. QI in healthcare subsequently emerged internationally as a field, with a corresponding academic and evaluation community.16 Furthermore, the environmental impacts of healthcare have not been widely published until the last two decades.1 9 17
Study selection
Studies were included if they described a QI initiative or clinical innovation in the human healthcare setting that was intended to address environmental impact with at least one quantitative environmental sustainability metric. Intention was determined with reference to the study’s stated aim, rationale and conclusions. Sustainability metrics were considered broadly, including environmental impact data, which measure emissions and waste associated with the production or consumption of resources (eg, kilograms of CO2) and activity data, which are comparable to process or structure measures in QI and can serve as a proxy for environmental impact (eg, vials of drug used).
We excluded modelling studies, reviews, case reports, editorials, letters, commentaries and other publications that did not report any primary data or present new analyses of existing data. Studies describing QI or clinical innovation efforts taking place in the healthcare setting but outside of the clinical encounter (ie, physical plant, exclusively operations or engineering) were also excluded. Studies that were not peer reviewed or published in languages other than English were also excluded.
Covidence was used to screen search results and extract data. A team of four reviewers (KB, CSCL, DH, SY) conducted a two-stage screening process. The first stage was abstract and title review, with eligibility confirmed by two independent reviewers. Disagreements were resolved through discussion and consensus, involving a third reviewer if consensus was not achieved. The second screening stage was conducted on full-text articles with the four initial reviewers (KB, CSCL, DH, SY) and an additional reviewer (DB), again in duplicate with disagreements resolved through discussion and consensus; an additional reviewer was involved if consensus was not achieved.
Data extraction
Data were extracted in duplicate by two independent reviewers using a pilot-tested data abstraction form in Excel. Abstracted data were grouped into three categories—publication, study and measurement characteristics. The publication characteristics captured the title, publication year, abstract/full text, study duration, first author and journal. Study characteristics include the country of origin, inpatient/outpatient setting, clinical specialty, study design, funding source, type of QI intervention used and broad categorisation within the sustainability framework of recycle, reduce and reuse. This framework was selected as it has been promoted by environmental organisations and governments for decades as a simple and memorable way to encourage sustainable behaviour in everyday life.
Data charting
We charted the extracted data both narratively and quantitatively using tables and figures. We categorised QI interventions based on a typology of QI interventions in the resource stewardship literature.18 Measurement characteristics captured each metric across the included studies. For each metric, we noted whether the sustainability metric tracked activity data (eg, vials of medication used) or environmental impact data (eg, GWP). We also noted whether the metric’s scale was absolute (ie, kilogram waste reduction), relative (ie, percentage waste reduction) or both, and the unit of measurements used to quantify each metric (eg, kilogram, litre, etc). Multiple metrics could be charted from a single study, so proportions for metrics often sum to greater than 100%.
Results
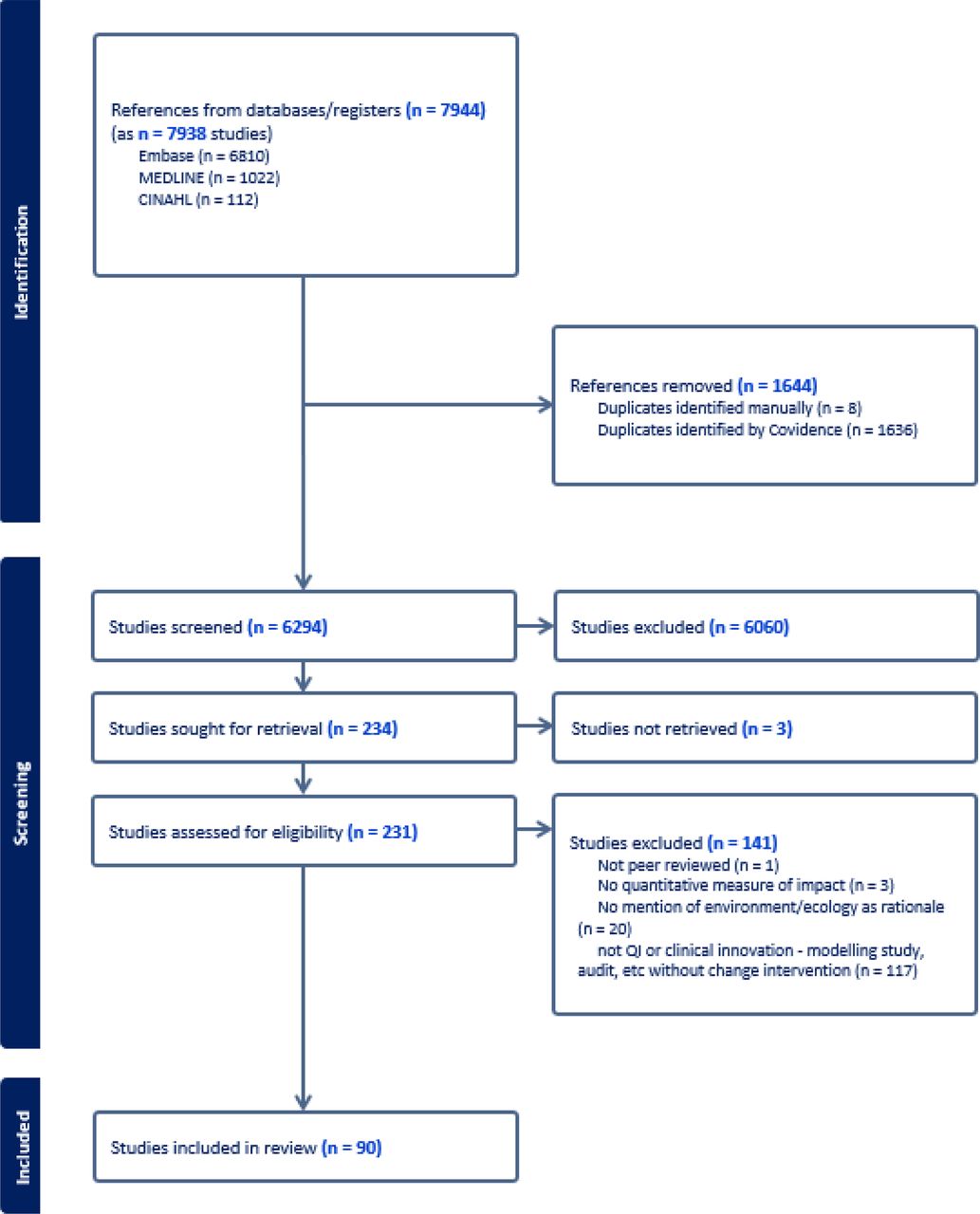
The search strategy identified 6294 unique references. After completing our two-stage screening process, we ultimately included 90 publications (figure 1, online supplemental table 2). Of these, 66% (59/90) were full publications and 34% (31/90) were conference abstracts. Study characteristics are presented in table 1.
Supplemental material
Study characteristics

Study selection based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram, available online (www.prismastatement.org). QI, quality improvement.
We identified a significant increase in published QI initiatives addressing environmental sustainability between 2019 and 2023 (online supplemental figure 1). Publications originated predominantly from the United Kingdom (41%, 37/90) and the USA (32%, 29/90), with all other countries contributing fewer than 10% of included publications each (online supplemental table 3). A plurality of publications documented an intervention taking place over less than a year. Identified publications were predominantly published in specialty journals rather than journals dedicated to QI. The majority of studies (83%, 75/90) used a before–after design to analyse the effectiveness of their QI intervention or clinical innovation. Funding was uncommonly reported. When it was, publications were typically not funded (54%, 22/41 studies identifying any funding source).
Supplemental material
Supplemental material
We found QI interventions across medical, surgical and allied health disciplines, generally reporting on initiatives carried out in the inpatient setting (78%, 70/90), with the highest percentage of publications arising from anaesthesiology (40%, 36/90) (table 2). These studies mostly featured interventions to reduce and eliminate the use of the highly volatile inhaled anaesthetic gas desflurane, which has an outsized environmental footprint due to its long atmospheric lifespan and energy-intensive production. Anaesthesia studies also included interventions to substitute anaesthetics or change practices, such as introducing low flow gas rates, which release less gas during procedures. Nearly all QI interventions and clinical innovations aimed to reduce the volume of an environmentally consequential practice (98%, 88/90), whereas reuse and recycling were far less commonly the focus (11%, 10/90 and 19%, 17/90, respectively).
QI interventions used
Included studies generally used a multicomponent approach to their QI intervention, which the resource stewardship literature has identified are more effective in addressing the complexity of reducing unnecessary healthcare (69%, 62/90)(table 2). Among the deployed QI interventions, the most common were creating a new clinical pathway for care or establishing new criteria for discontinuation of a service (63%, 57/90), clinician education (60%, 54/90), audit and feedback (27%, 24/90), recommendation or guideline dissemination to clinicians (27%, 24/90) and behavioural nudges (26%, 23/90). No studies used any form of clinician risk-sharing or patient cost-sharing.
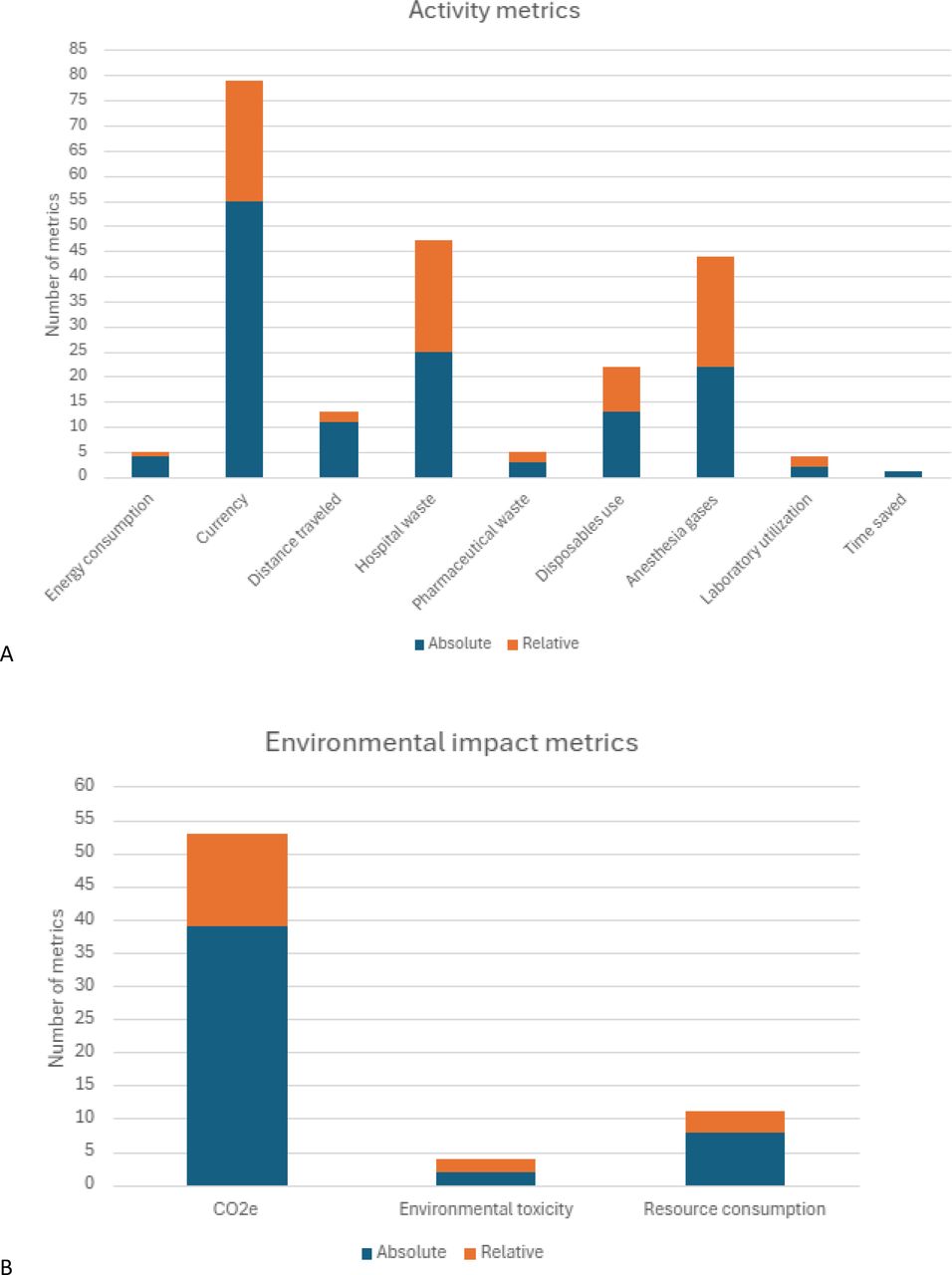
Sustainability metrics targeted both activity data and environmental impacts. Studies predominantly reported activity data. These were aggregated into eight categories, listed in order of relative frequency: cost, hospital waste, anaesthetic gases, disposables used, distance travelled, pharmaceutical waste, laboratory utilisation and other (figure 2A). Fewer publications reported environmental impacts (figure 2B). Of those that did, GWP as measured by greenhouse gas emissions was overwhelmingly the impact category of choice. Studies tended to report absolute rather than relative changes in their metrics. We chose to consider the widespread use of financial cost as an activity measure related to sustainability, which may be criticised as an overly indirect or general metric. However, it is well justified on the basis that, on the time horizon used for the included studies, financial cost is a good proxy for environmental impacts.19

{kind=link}
{kind=link}
Bar charts illustrating (A) activity metrics and (B) environmental impact metrics. The unit of analysis is the individual metric reported, rather than the study, so the number of metrics is greater than the number of studies.
The diversity of ways in which a single environmental impact indicator could be operationalised is summarised in table 3. For example, utilisation of anaesthetic gases was most commonly quantified by volume of gases used in litres, but some studies used flow rates and others used vials of medication disposed.20 21 Hospital waste was most commonly quantified by the weight of waste, but some studies measured the proportion of waste that was recycled, incinerated as hazardous waste or disposed of as solid waste.22 23
Measures for frequently reported sustainability metrics
Discussion
In this scoping review of published QI interventions and clinical innovations intended to address environmental sustainability in the clinical setting, we identified 90 publications utilising a range of QI approaches and sustainability metrics. Our results complement those of the recent scoping review by Padget et al that found ‘environmentally sustainable healthcare’ to be a heterogeneous concept as used by studies that either defined environmentally sustainable healthcare or measured the impact of healthcare on the environment.10 One might expect those taking action on environmental sustainability in healthcare, as potential leaders in the space, to embrace more consistent approaches to the concept and its measurement. Our review of published QI initiatives demonstrates that this is not the case. Heterogeneity in the broader sustainable healthcare literature is mirrored in the way that QI initiatives have been undertaken and measured. We found an opportunistic use of available measures, with activity measures (eg, number of vials used) serving as proxies for environmental impact, and waste in particular. The field of healthcare environmental impact measurement is rapidly evolving, through the increased expansion and application of life cycle assessments across a broader range of delivery activities. Over time, it is anticipated that these advancements will enhance confidence in approaches to measuring the effectiveness of interventions in achieving intended environmental impacts.
Within the included studies, interventions to reduce and reuse dominated those aimed to promote recycling. This relative de-emphasis of recycling is in line with growing evidence in the literature that recycling is of marginal impact for mitigating environmental harms of healthcare.20 The reporting of absolute change in metrics of environmental harm is more meaningful than relative change, the latter of which can fall into a trap of improving efficiency (environmental harm-per-unit) while increasing environmental harm overall.24 In these respects, it appears that the body of QI efforts targeting environmental sustainability demonstrates a general adherence to best practices in QI.
Nonetheless, our review findings illustrate that QI efforts directed at environmental sustainability are at risk of suffering from ‘carbon tunnel vision’, a term describing the tendency to optimise for climate change to the exclusion of considering other environmental impacts. GWP was by far the most common environmental impact reported, but other environmental impacts were uncommonly reported or never reported (eg, particulate matter formation, eutrophication potential, ozone depletion). ‘Carbon tunnel vision’, as we see in our review findings, can obscure the potential for interventions to worsen other environmental impacts, even as they improve GWP. Some have theorised that national and organisational targets to reduce carbon emissions have led to other environmental impact measures to be overlooked in healthcare.10 Environmental measures are complex and require input from diverse experts in sustainability science, waste management and engineering, among others. For environmental sustainability QI work in particular, engaging such experts in these fields to access or leverage meaningful data to test, evaluate and guide changes is critical. While vast amounts of data are gathered in healthcare organisations, much of it is not readily available in timely or usable formats to support meaningful QI.25
The United Kingdom published more QI studies than any other country. In the context of the NHS being the first national health system to declare a net zero pathway, this speaks to the power of high-level political commitment to sustainability. In the case of the NHS, this has translated to a culture of sustainability aligned with QI in the NHS, driven both by a critical mass of interested individual scholars as well as institutional leadership.26 There is a robust network of researchers, organisations and teams in the UK that align environmental sustainability with QI through the Sustainable Quality Improvement (SusQI) framework.27 28 SusQI integrates environmental, social and economic sustainability into traditional QI processes. SusQI expands the definition of value in healthcare by considering not only clinical outcomes and cost-effectiveness but also the environmental and social impacts of care delivery.1 Efforts to date have included courses in sustainable QI as well as establishing specialty-specific communities of practice.29
Globally, there is a need to spread this agenda through the QI academic and practice communities. Advancing measurement of environmentally sustainable QI involves capacity building in QI education and practice. By aligning this environmental sustainability, QI measurement frameworks with other QI elements of goal setting, systems thinking and improvement methods, data proficiency related to environmental sustainability can be rapidly incorporated in mainstream QI training programmes.1 29 Furthermore, professional bodies and educational institutions can encourage capacity building by introducing sustainability-focused sections to conferences, awards or journals. Advancing individual QI capacity building on environmental sustainability can facilitate organisations to include environmentally focused QI measures as part of hospital strategic quality plans, which may also drive governments to establish sustainability targets, or be motivated by such targets. QI scholarship can also be supported through the development of updated publication guidelines such as SQUIRE to provide a framework for reporting and publication, to help advance the field and share QI work through scholarly platforms such as specialty-specific and QI-focused journals.30 31
Our conclusions are strengthened by our rigorous methodological choices and cross-disciplinary collaboration within the authorship group. The group includes diverse scholars with expertise in evidence synthesis, QI and environmental impact analysis alongside expertise in surgery and internal medicine. The scoping approach provided us with the latitude necessary to characterise an emerging, heterogeneous body of literature. We used a broad search strategy designed in collaboration with an expert information specialist and screened over 6000 titles to arrive at our included studies.
Our study has several limitations. We restricted our search to publications in English. Our sample of QI interventions is therefore most representative of efforts taking place in regions where clinicians publish in English. However, language restrictions have been shown to not have deleterious effects on the results of systematic reviews, so it may be reasonable to extrapolate our results outside of English-speaking countries.32 Furthermore, our focus on English-language studies is aligned with our aim to hold a mirror to the sustainability efforts of QI thought leaders and scholars, who are primarily stationed in the predominantly English-speaking global north. Consistent with the scoping review approach and our overall study aims, we did not evaluate the quality of the included publications nor appraise the effectiveness of their interventions. Given the volume of included studies, we charted data elements as reported by the study authors without contacting them for clarification. This meant that we were limited in our capacity to comment on some characteristics of QI initiatives that authors chose not to report in the text of the included studies (eg, description of outcomes as measures of improvement vs balancing measures). Some may question how we identified QI interventions and clinical innovations intended to address environmental sustainability. Our aim was to write about and for the community of QI practitioners with an interest in environmental sustainability. We recognise that we will not have included QI interventions that may have had salutary environmental impacts without intending to, and we may have included other QI interventions where their environmental rationale was only added post-hoc. Sorting these out—in particular the latter—would be prohibitively difficult. Our approach leaves us with a body of literature that would be drawn on by those hoping to produce additional surveys of the field or launch their own QI initiative. Finally, we did not include a grey literature search within the scoping review.10 We identified an abundant number of studies with our conventional database search, and resource limitations meant that we could not pursue a grey literature search. It can be a challenge to publish QI efforts in the academic literature, and there are often institutional or local toolkits developed to share this information, as such representing an opportunity for a broader literature search.
Conclusion
Clinicians are increasingly turning their attention to the environmental crisis by bringing environmental sustainability into the clinical realm using the familiar methods of QI and clinical innovation. Existing efforts are predominantly from the United Kingdom, produced by the discipline of anaesthesiology and focused on climate impacts. There is an opportunity and a need for greater engagement from other clinical disciplines. Clinicians engaged in this work are becoming increasingly conversant with a broader family of measures in QI beyond clinical outcomes. Future QI and clinical innovation scholarship and practice should incorporate feasible environmental metrics, guided by scholarly guidelines and collaboration with diverse experts who have insights and access to sustainability measures. Ideally, these QI efforts will be embedded in settings with policies that recognise the interconnectedness of healthcare quality and environmental sustainability.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Footnotes
X @Brian_M_Wong, @bornk
Contributors KBB conceived the scoping review and is responsible for the overall content as guarantor. CS-C-L, SY, DH, DB and KBB contributed actively to the scoping review activities as well as drafting the manuscript. CS-C-L, SY, DMH, DB, BMW, NS and KBB contributed to analysis of findings and editing of the manuscript.
Funding This study was funded through a University of Toronto Dalla Lana School Public Health (DLSPH) Implementation Science Interdisciplinary Research Cluster seed grant.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer-reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.