Article Text

Abstract
The continued use of low-value cancer screening practices not only represents healthcare waste but also a potential cascade of invasive diagnostic procedures and patient anxiety and distress. While prior research has shown it takes an average of 15 years to implement evidence-based practices in cancer control, little is known about how long it takes to de-implement low-value cancer screening practices. We reviewed evidence on six United States Preventive Services Task Force ‘Grade D’ cancer screening practices: (1) cervical cancer screening in women<21 years and >65 years, (2) prostate cancer screening in men≥70 years and (3) ovarian, (4) thyroid, (5) testicular and (6) pancreatic cancer screening in asymptomatic adults. We measured the time from a landmark publication supporting the guideline publication and subsequent de-implementation, defined as a 50% reduction in the use of the practice in routine care. The pace of de-implementation was assessed using nationally representative surveillance systems and peer-reviewed literature from the USA. We found the time to de-implementation of cervical cancer screening was 4 years for women<21 and 16 years for women>65. Prostate screening in men ≥70 has not reached a 50% reduction in use since the 2012 guideline release. We did not identify sufficient evidence to measure the time to de-implementation for ovarian, thyroid, testicular and pancreatic cancer screening in asymptomatic adults. Surveillance of low-value cancer screening is sparse, posing a clear barrier to tracking the de-implementation of these screening practices. Improving the systematic measurement of low-value cancer control practices is imperative for assessing the impact of de-implementation on patient outcomes, healthcare delivery and healthcare costs.
- Implementation science
- Quality measurement
- Standards of care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The continued use of low-value clinical practices diminishes healthcare quality and exacerbates healthcare costs.1 A low-value practice refers to care that provides little or no benefit, is costly or is potentially harmful.2 Wasteful spending accounts for approximately 25% of US healthcare costs, with low-value care representing an estimated US$75–100 billion in annual expenditures.3 In the context of the cancer care continuum, the use of low-value practices is widespread and contributes to the rising cost of cancer care.4–7 For cancer screening in particular, the use of low-value practices not only represents healthcare waste but also a potential cascade of invasive diagnostic procedures and significant patient anxiety and distress.8
De-implementation refers to the systematic discontinuation or reduction of a service or practice that is ineffective, unproven or harmful. The de-implementation of low-value practices is hampered by multilevel barriers, including poor dissemination of evidence, entrenched norms and resistance to change, confusion and scepticism resulting from frequent changes in practice guidelines and patient expectations.9 10 Further complicating the issue is the need for personalised care and shared decision-making, which may call for the selective use of a low-value practice in certain patients.10 11 The de-implementation of low-value practices can also result in unintended consequences such as reduced health system revenue, inappropriate utilisation of other practices and loss of patient trust.12 Although de-implementation strategies have been extensively studied for practices such as inappropriate antibiotic and opioid prescribing, evidence on the de-implementation of low-value cancer screening is scarce.13
Khan et al demonstrated that it takes an average of 15 years from the publication of a landmark study for five evidence-based practices in cancer control to achieve 50% uptake in practice.14 For example, they found the time from the publication of clinical trials demonstrating the efficacy of a practice to reaching 50% uptake was 21 years for mammography and 14 years for human papillomavirus (HPV) vaccination. In contrast, little is known about how long it takes to de-implement low-value cancer control practices.15 16 To address this gap, we aimed to (1) describe the availability of evidence on the de-implementation of low-value cancer screening practices in routine care in the USA and (2) measure the time to de-implementation of these practices in routine care.
Methods
We reviewed the United States Preventive Services Task Force (USPSTF) clinical practice guidelines to identify clinic-based low-value cancer screening practices.17 The USPSTF assigns each guideline a grade on an ‘A’ to ‘D’ scale, with practices with insufficient evidence to assess being graded as an ‘I’. A Grade D guideline indicates a recommendation against delivering a practice based on moderate or high certainty the service has no net benefit or that the harms outweigh the benefits. The guidelines are accompanied by published systematic evidence reviews that present the evidence base and rationale for each recommendation. As of 2023, the USPSTF Grade D services included six clinic-based cancer screening practices: (1) cervical cancer screening in women<21 years and >65 years, (2) prostate-specific antigen (PSA)-based prostate cancer screening in men≥70 years and screening of asymptomatic adults for (3) ovarian, (4) thyroid, (5) testicular and (6) pancreatic cancer. Table 1 presents the history of the current USPSTF Grade D practices and their associated screening tests and procedures as described in USPSTF guidelines.
Current United States Preventive Services Task Force (USPSTF) Grade D cancer screening practices and preceding USPSTF recommendations
To assess the availability of evidence on de-implementation in routine clinical practice, we reviewed documentation from five publicly available US surveillance datasets: the Healthcare Effectiveness Data and Information Set (HEDIS),18 Medical Expenditure Panel Survey,19 Behavioral Risk Factor Surveillance System,20 National Health Interview Survey20 and the National Health and Nutrition Examination Survey.21
We adapted the approach used by Khan et al14 to assess the time to de-implementation of the selected low-value cancer screening practices. This approach takes into account both the time it takes for published evidence to be incorporated into clinical practice guidelines and the time required for these guidelines to be adopted in real-world practice. We measured the time from (1) the landmark publication(s) cited in the USPSTF guideline and evidence review (eg, first randomised controlled trial (RCT) demonstrating either null results or harms that outweigh benefits) to (2) USPSTF guideline release and (3) subsequent de-implementation of the practice in routine clinical care. If the guideline cited a cumulative body of evidence rather than a landmark study, we used the year of the most recent publication that supported the recommendation statement. As there is no universal threshold for successful de-implementation, we define de-implementation as a 50% reduction in the use of a practice in routine care, following the approach used by Khan et al.14
We reviewed published literature to assess the de-implementation of the cancer screening practices in routine care. We included studies that were peer-reviewed, used nationally representative US data and included data from both pre-guideline and post-guideline time periods. For studies reporting nationally representative data, we considered evidence from national claims data (eg, Medicare), nationally representative surveys and studies using medical record data from multiple health systems and/or geographic regions. We searched Embase using terms for each screening practice combined with search terms for low-value care, USPSTF guidelines and de-implementation (see online supplemental appendix A). Two authors (JL, KP) reviewed the resulting title and abstracts to identify potentially relevant literature. Reference lists were also examined to identify additional studies.
Supplemental material
Results
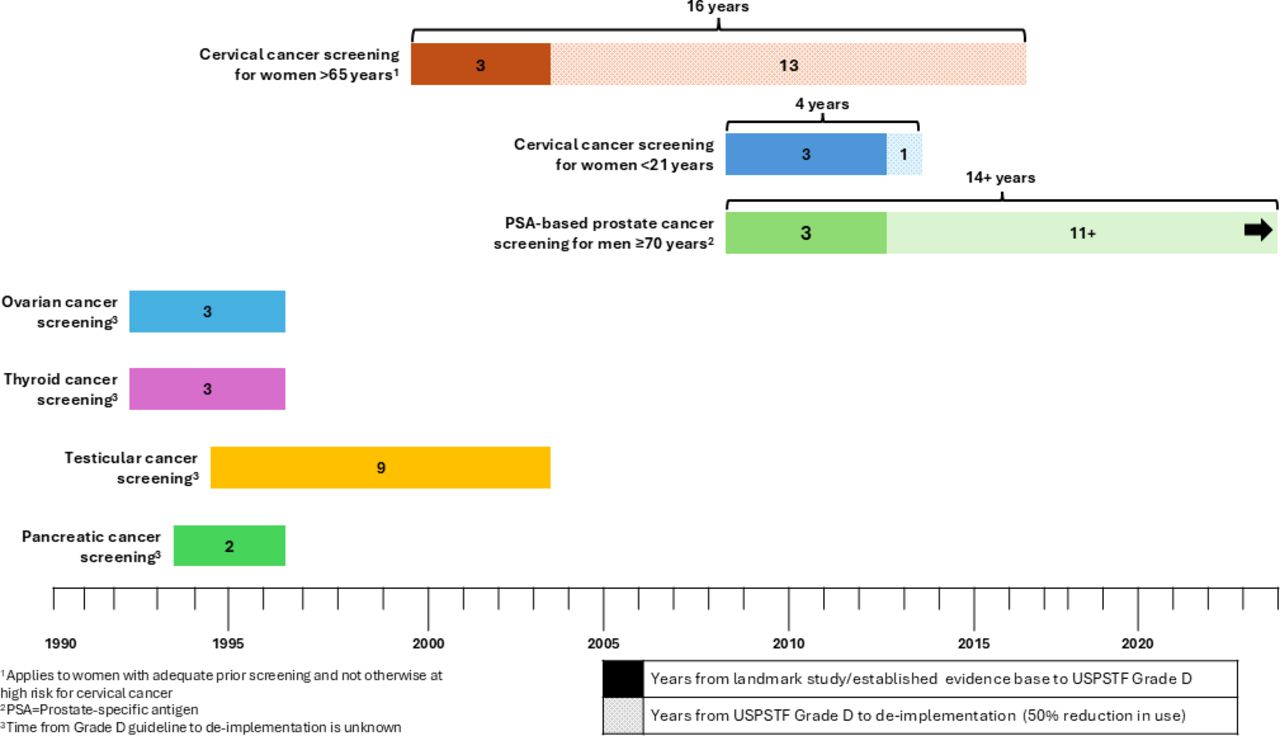
Nationally representative estimates of screening practices were only available for prostate and cervical cancer screening. Research on the use of the other practices was limited by single-centre studies, non-representative samples and a lack of pre-guideline data. The current evidence on time to de-implementation for each practice is summarised in figure 1. The annual low-value screening rates for cervical and prostate cancer reported in each included study are summarised in online supplemental appendix B.

{kind=link}
Time to de-implementation of selected USPSTF Grade D cancer screening practices. USPSTF, United States Preventive Services Task Force.
Cervical cancer screening
Screening in women under 21 years
The USPSTF assigned a Grade D recommendation for cervical cancer screening in women under 21 years in 2012 and reaffirmed this rating in the subsequent 2018 guideline.22 23 The evidence review cited a body of evidence to support this decision, noting the strongest evidence came from a case–control study published in 200924 and was supported by previous cohort studies.25–28 Two studies observed a reduction in screening of over 50% from 2011 to 2013.29 30 A study using a nationally representative sample of US office-based medical visits found screening rates fell from 4.3% in 2011 to 1.6% in 2013 among women aged 14–20 years and from 8.3% to 3.0% among women aged 18–20 years, with patients residing in the Southern US and those with public insurance more likely to be screened.29 Similarly, another study using patient data from three large health systems (n=55 316) showed screening rates in women aged 18–20 years declined from 8.3% in 2011 to 2.4% in 2013, though without variation by geographic region, healthcare system or patient characteristics.30 A HEDIS healthcare quality measure introduced after the 2012 guideline shows the rate of non-recommended screening among women aged 16–20 years was <1.0% in 2022.31 Overall, these findings show a 4-year time to de-implementation (2009–2013), including a 3-year gap between the landmark 2009 study and the 2012 USPSTF guideline release, followed by an over 50% reduction from pre-guideline screening rates in 2013.
Screening in women over 65 years
The 2003 USPSTF Grade D recommendation for cervical cancer screening in women over 65 years was first issued in 2003 and reaffirmed in 2012 and 2018.22 23 32 The original Grade D was based on evidence from 12 observational studies published between 1995 and 2000 rather than a single landmark study.32 33 In an analysis of Medicare claims data, Qin et al found screening rates reached a relative reduction of 50.5% in 2016 (19.0% in 2002 to 9.4% in 2016), 14 years after the guideline was issued.34 The observed trends were consistent across race and ethnicity, although the age-adjusted rate of screening was consistently highest in non-Hispanic white women. Although this study was unable to determine if women had prior adequate screening, hysterectomy or a history of cervical cancer or abnormal screening results, to our knowledge it is the only study using a national US sample with an observation period encompassing pre-guideline and post-guideline screening rates. In summary, the time to de-implementation of cervical cancer screening in women over age 65 spanned 16 years, with 3 years between the publication of supporting evidence and guideline release (2000–2003) and another 13 years between the guideline release and 50% reduction in screening (2003–2016).
PSA-based prostate cancer screening in men aged 70 years and older
As shown in table 1, USPSTF guideline recommendations for prostate cancer have fluctuated over the years. A Grade D has been maintained for men aged≥75 years since the 2008 USTPF guideline, which cited a 2005 study to support the recommendation. For men aged≥70 years, a Grade D rating has been in effect since the 2012 guideline. The USPSTF released a draft of this guideline in 2011 for public comment, citing the results of two large trials, both published in 2009, as the primary evidence for the Grade D rating.35–37 Longer-term follow-up results from both trials were published in 2012, shortly before the final guideline was released.38 39 The USPSTF concluded these new results supported the previous findings and published the final version of the Grade D rating in 2012.40 41
Several studies using nationally representative survey and administrative claims data have demonstrated initial modest (<20%) reductions in low-value prostate cancer screening among men aged≥70 years following the 2008 and 2012 recommendations.42–50 More recent data show an increase in low-value screening after 2016.51–53 Zhu et al51 found rates of screening among Medicare Advantage enrollees aged 70–74 years initially declined after the 2012 recommendation statement from 37.0% in 2011 to a low of 32.8% in 2015, but by 2019 rates had increased to 50.3%; a similar pattern was observed among men aged≥75 (24.3% in 2011, 21.3% in 2015 and 34.8% in 2019). Studies using self-reported survey data found consistently higher screening rates than those using claims data (online supplemental appendix B). The most recent HEDIS data show that approximately 30% of men aged≥70 years still receive non-recommended screening in 2022.54 These findings demonstrate that while the time from landmark study publication to guideline release was 3 years (2009–2012), the practice has yet to reach the 50% threshold for de-implementation more than 11 years after the guideline publication.
Ovarian cancer screening in asymptomatic women
The 1996 ovarian cancer screening Grade D guideline cited studies published in 1990, 1991 and 1993 showing no benefit of pelvic screening, serum tumour testing and transvaginal ultrasound screening methods.55–58 Subsequent USPSTF guidelines cited two large RCTs published in 2011 and 2016 to support the continuation of the Grade D rating.59–62 Two national surveys measured physician-reported ovarian cancer screening practices after the guideline publication. A 2012 survey of women’s primary care physicians (n=1088, response rate 61.7%) found that 28% of respondents reported performing inappropriate screening.63 Similarly, a 2016 survey of gynaecologists (n=401, response rate 67.1%) found that 58% of respondents reported regularly recommending inappropriate screening.64 Given the lack of evidence on pre-guideline practice trends, our characterisation of the time to de-implementation is limited to the 3 years between the publication of evidence demonstrating the lack of benefit of screening (1993) and the release of the USPSTF guidelines (1996).
Thyroid cancer screening in asymptomatic adults
The Grade D recommendation for thyroid cancer screening was issued in 1996 and cited studies published as late as 1992. The recommendation statement described a lack of evidence for screening benefits and poor accuracy of available screening methods.65 The 2017 guideline evidence review also found insufficient evidence to support screening for thyroid cancer in asymptomatic adults or children.66 67 A meta-analysis of seven single-centre observational studies published between 1998 and 2019 found the pooled frequency of inappropriate thyroid ultrasound screening was 46% (95% CI 15% to 82%).68 Because the measurement of real-world practice is limited to single-centre studies, we can only identify the 3-year gap between the most recent publication cited in the original guidelines (1993) and the corresponding guideline release (1996).
Testicular cancer screening in asymptomatic adolescent and adult men
The USPSTF issued a 2004 Grade D recommendation for testicular cancer screening in 2004 due to the low incidence and high cure rate of testicular cancer, potential for false positives leading to invasive diagnostic procedures and a lack of evidence on the accuracy of screening tests and screening outcomes.69 The recommendation was updated from the 1996 Grade C rating due to changes in the USPSTF methodology and rating system rather than new evidence.69–71 The 1996 USTPF statement cited evidence published up to 1995.72 To our knowledge, no studies have produced representative estimates of testicular cancer screening practices over time.73 74 Therefore, we are only able to measure the 9-year span between the publication of evidence (1995) and Grade D recommendation (2004).
Pancreatic cancer screening in asymptomatic adults
A Grade D recommendation was issued in 1996 for pancreatic cancer screening based on inconclusive evidence for improved morbidity and mortality from early detection, the absence of reliable screening tests, high false positive rates and need for invasive diagnostic procedures.75 The guideline statement cited studies published as late as 1994.75 The Grade D recommendation was upheld through updated evidence reviews in 2004 and 2019.76 77 To our knowledge, no published research exploring screening rates for pancreatic cancer in the USA is available. Therefore, we are only able to measure the 2-year gap between supporting evidence (1994) and the publication of the guideline (1996).
Discussion
Our examination of six USPSTF Grade D cancer screening practices enabled us to measure the time to de-implementation for low-value cervical and prostate cancer screening. The lack of data for the four remaining practices illustrates the pronounced challenges in measuring the time to de-implementation of low-value cancer screening practices. Although the availability of HEDIS quality indicators for cervical and prostate cancer screening represents significant progress in measuring low-value practices, the lack of available measures to track the use of the four other screening practices demonstrates the need for increased attention at the national level. Given the substantial cost, reduction in healthcare efficiency and patient harm that results from low-value cancer screening, there is a clear need to improve the monitoring and active de-implementation of these practices.
Valid and accessible measures and data sources with sufficient granularity to monitor the delivery of low-value care practices are needed to set benchmarks and monitor de-implementation efforts.78 The vast majority of clinical performance measures address the underuse of evidence-based practices rather than the overuse of low-value care,79 and most existing low-value measures focus on treatment rather than screening and prevention services.80 The fragmented nature of the US healthcare system makes obtaining representative population data particularly challenging. Administrative data are limited to the included health plans, nationally representative surveys are subject to recall and social desirability bias and both approaches have limited specificity in the absence of linked medical record data and highly detailed measure definitions.81 82 Chart review comes closest to a ‘gold standard’ measurement approach but is impractical to conduct even in a single health system. In addition, compared with practices with clear age guidelines and specific tests (eg, PSA and Pap testing in selected age groups), the details of a physical examination or intention of a diagnostic test are more challenging to obtain from electronic health records or administrative data. In these cases, artificial intelligence holds promise in overcoming the limitations of other methods.83 For the time being, expanding the representation of low-value practices in healthcare quality metrics and large national surveys is the most feasible approach for standardised monitoring of low-value care.
Khan et al found that the time from the publication of a landmark study to implementation (defined as 50% uptake) of five cancer control practices ranged from 13 to 21 years. Among the three cancer screening practices, the time to implementation was 14 years for Pap and HPV co-testing in women aged 30–65, 15 years for colorectal cancer screening in adults aged 50–75 and 21 years for mammography in women aged 50–74.14 In contrast, we found the time to a 50% reduction in low-value cervical cancer screening in women under age 21 and over age 65 ranged from 4 to 16 years.29 30 34 This range in time to de-implementation may prove even more pronounced given that prostate cancer screening rates in men aged 70 and older have not reached this threshold after 14 years, and rates have remained relatively unchanged since 2015.54
Several explanations exist for the varying pace of de-implementation. First, pre-guideline rates of cervical cancer screening in women under 21 years were lower than cervical or prostate cancer screening in older adults, thus requiring less time to de-implement.29 30 34 84 Second, while most primary care providers are familiar with the USPSTF recommendations, other providers are more likely to adhere to guidelines from professional bodies specific to their specialty.85 The American Congress of Obstetricians and Gynecologists issued recommendations to delay screening until age 21 in 2009,86 likely contributing to a decline in screening women under 21 years before the 2012 USPSTF guideline release.87 For prostate cancer screening, the current USPSTF recommendations diverge from those of other societies and have been the subject of controversy.88–90 Further, age-based prostate cancer screening recommendations have changed frequently over the past two decades.40 65 91–93 Finally, healthcare providers may encounter more resistance from patients when a previously received screening is discontinued compared with the delayed initiation of screening. The variation in the pace of de-implementation of these practices points to the need for de-implementation strategies tailored to both the low-value practice and the setting in which it is delivered.
Conclusion
Surveillance of low-value cancer screening is sparse and inconsistent, posing a clear barrier to effectively tracking the de-implementation of these screening practices. Although national quality measures are available for select low-value cancer screening practices, we identified a clear need to develop better infrastructure to systematically monitor their use. Further, the significant timeframe for de-implementation of low-value cancer screening practices demonstrates a need to employ deliberate de-implementation strategies rather than relying on publication of clinical guidelines alone. Increasing the use of evidence-based de-implementation strategies coupled with improved measurement of low-value cancer control practices is imperative for improving patient outcomes, reducing healthcare costs and increasing healthcare system efficiency.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Footnotes
Contributors JL and KP contributed to the conceptualisation, data curation, formal analysis, investigation, writing of the original draft and funding acquisition this project. RS and NSO contributed to the conceptualisation. RS, NSO and WN contributed to writing—review and editing. JL is the guarantor.
Funding This study received funding from National Cancer Institute's Consortium for Cancer Implementation Science.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.