Article Text

Statistics from Altmetric.com
- healthcare quality improvement
- continuing education, continuing professional development
- implementation science
- shared decision making
Tackling overuse in healthcare is now more necessary than ever. Movements such as Choosing Wisely and Preventing Overdiagnosis have highlighted that some healthcare services offer no added value and may even cause harm to patients. Estimates of overdiagnosis and overtreatment vary widely between services, providers and regions.1 2 Overuse is a persistent challenge in high-income countries and is increasingly recognised in low-income settings.3 Action is needed to prevent patient harm, reduce resource waste and preserve the limited time of healthcare professionals. In addition, since healthcare services have a significant environmental impact, minimising overuse can contribute to achieving climate goals.
De-implementation science
To accelerate the reduction of overuse, robust de-implementation science is essential.4 This field studies the drivers, strategies and processes involved in reducing or eliminating ineffective, unnecessary or harmful healthcare practices, and in replacing them with evidence-based, high-value alternatives. Rigorous studies have identified several causes of overuse across different levels. Physicians often feel pressured by peers, patients and the broader medical culture to intervene, even when treatment is unnecessary.5 Patients may have high expectations, often shaped by unreliable health information.6 Additionally, healthcare systems include incentives that promote low-value care—such as the payment system and the aggressive marketing strategies of the pharmaceutical and medical device industries—which help sustain a ‘more is better’ culture.7 Since the launch of Choosing Wisely in 2012, there has been a modest but growing number of studies on de-implementation. A PubMed search shows no results for ‘de-implementation OR deimplementation’ in 2013, compared with 89 in 2024. A key challenge in de-implementation science is designing and implementing effective strategies for reducing low-value care.8
Patient requests
A study published in this issue of BMJ Quality and Safety9 explores why physicians continue to provide low-value care. Using a factorial survey experiment among 593 Swedish primary care physicians, the researchers found that physicians’ perceptions of patient requests and their positive perceptions of the clinical practice in question increased the likelihood of providing low-value care by 14 and 13 percentage points, respectively. When the low-value intervention required minimal time or cost, patient requests became even more influential, increasing the likelihood by 29 and 18 percentage points, respectively. However, when physicians were presented with credible evidence identifying an intervention as low value, the influence of patient requests decreased by 11 percentage points. The authors suggest that improved knowledge, communication tools and decision-support systems incorporating guidelines are crucial for reducing low-value care.
Self-reflection
This study highlights that many physicians think that patients play a major role in driving low-value care. However, it is noteworthy that physicians often emphasise this factor while overlooking other important determinants at the level of healthcare professionals themselves. An evidence synthesis found that the majority of barriers to de-implementation occur at the provider level, including attitudes, knowledge, skills and behaviours.10 Still, physicians frequently assert that patients seek reassurance, yet research has shown that additional tests do not necessarily provide reassurance.11 They also point to system-level factors, such as fee-for-service payment models and the medical-industrial complex.7 While these factors are important, the many successful de-implementation initiatives within current systems suggest that reducing low-value care is achievable within any system. A Catalan initiative significantly reduced unnecessary prescriptions and imaging in primary care,12 and a Dutch national programme reduced several low-value healthcare services such as gastric endoscopies in young patients with dyspeptic complaints and follow-up consultations after treatment for basal cell carcinoma.13 Healthcare professionals must acknowledge that they are part of the problem—but also part of the solution. To effectively reduce low-value care, they need to recognise their role and actively engage in strategies that challenge entrenched practices and enhance clinical decision-making.
Shifting the culture
Healthcare professionals have developed numerous lists to identify and reduce non-evidence-based diagnostics and treatments. However, simply creating such lists does not lead to changes in medical practice.4 Healthcare professionals must be encouraged and motivated to apply these recommendations in daily practice. De-implementation science offers support by offering practical guidance for reducing overuse in clinical settings.14 Additional sources of inspiration include successful de-implementation initiatives that can be adapted to local contexts. By taking the lead in their organisations and practices, healthcare professionals can demonstrate the leadership necessary to drive the cultural shift: from a ‘more care is better’ towards thoughtful restraint and recognising that sometimes not intervening is the safest and most effective choice.
The principles of culture change
What might this cultural change look like?
1. Reframing the narrative: this culture change is not about reducing care or saving money.15 It is about reducing low-value care and replacing it with delivering high-value care, for example, not doing an arthroscopy in older patients with degenerative knee complaints, but offering physiotherapy, pain medication and specific advice on how to avoid these complaints. In these cases, high-value care means no specific interventions and explaining the rationale for restraint, acknowledging patient concerns and providing comfort. Several studies show that with appropriate communication, many patients prefer watchful waiting over immediate intervention.16
2. A new perspective on health and illness: the belief has grown that healthcare can solve all our problems, and that health is easily influenced by medical interventions. We have created huge expectations with major headlines about what physicians can do to improve our health. However, healthcare has a relatively limited impact on overall health compared with external factors such as socioeconomic conditions, individual behaviours—such as lifestyle choices—and genetic predisposition.17 It is essential that we emphasise the importance of lifestyle improvements, poverty reduction and social connectedness reducing loneliness alongside healthcare interventions.
3. Commitment to continuous learning: healthcare professionals should be open to learning and improving their practices. Learning networks, organised by professional associations can be invaluable. For example, Choosing Wisely Canada launched a national learning collaborative to tackle the overuse of laboratory tests in hospitals. Through this initiative, hospitals across the country joined a coordinated effort to curb low-value testing, allowing laboratory resources to be used more effectively.18 By sharing data, experiences and challenges in a safe environment, effective solutions can be disseminated from one region or country to another. An open mind to improve is conditional; we should avoid excessive debate about data quality and instead focus on learning through data comparison.
4. Resetting medical education and professional ethics: medical education must reinforce the principle that clinical restraint is a core component of high-value care. Latin maxims, such as ‘in dubio abstine’ (when in doubt, refrain) and ‘primum non nocere’ (first, do no harm), have been part of medical ethics since Hippocratic times and should continue to guide medical practice. Upholding these principles requires courageous supervisors who question why residents chose to order specific tests, rather than why they refrained from doing so.
Coalition of the willing
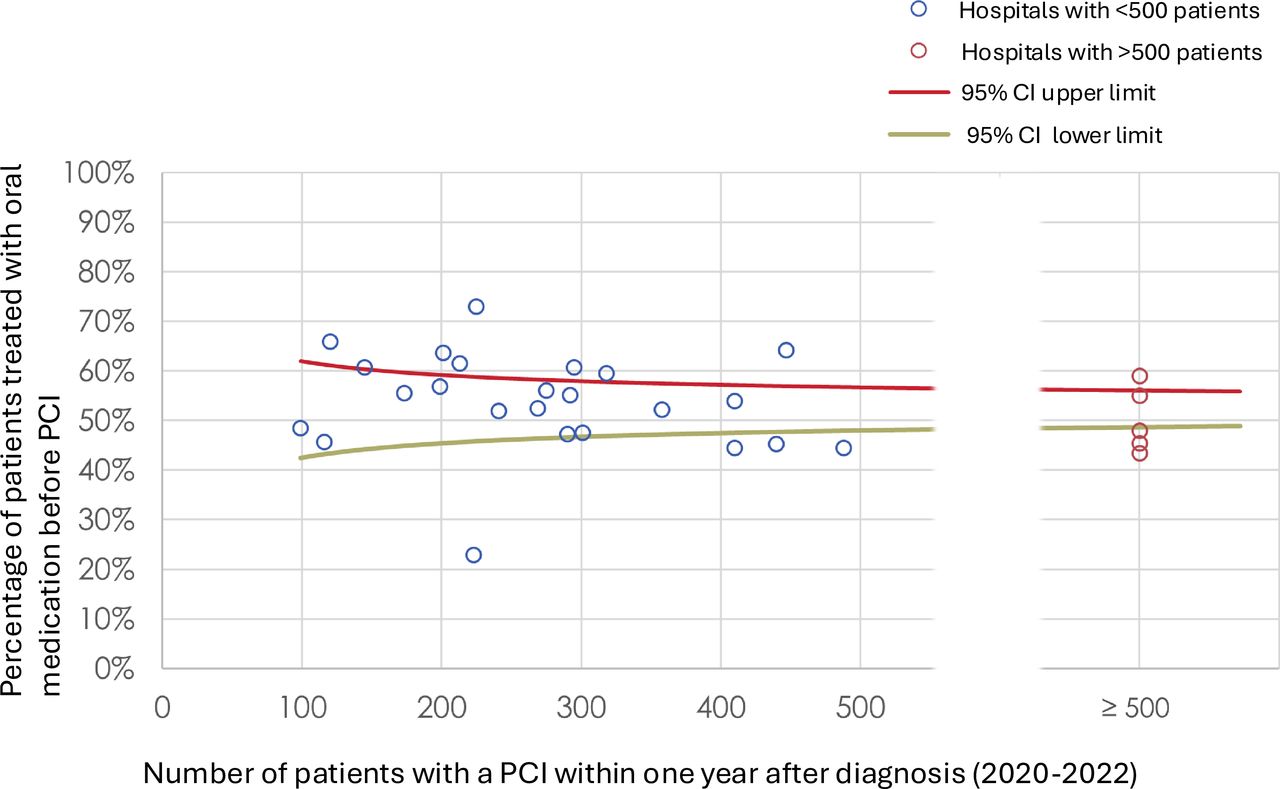
This culture shift is not the sole responsibility of healthcare professionals. De-implementation also requires system-wide changes. All relevant stakeholders must work together to foster a culture of continuous learning and improvement. In the Netherlands, such a coalition has been working together for 5 years to make healthcare quality improvement a routine part of daily medical practice. Objective benchmarking data on de-implementation plays a crucial role in this process. Dutch hospitals receive benchmark reports on various topics that are jointly prioritised by all stakeholders. The information is based on definitions formulated by a cooperation of healthcare professionals, insurers and the government to create broad support. Figure 1 shows an example of benchmark information about the treatment of stable angina pectoris, highlighting variations in adherence to guideline recommendations. On average, only 50% of these patients receive appropriate first-line oral medication. By contacting outliers and organising learning networks in which healthcare professionals share data, professional associations can organise a learning process to improve.

{kind=link}
Percentage of patients with stable angina pectoris who have been treated with oral medication before having a percutaneous coronary intervention (PCI).22
Communication skills
To drive cultural change, medical education must invest in developing the communication skills of healthcare professionals by integrating training on shared decision-making aimed at reducing low-value care. Shared decision-making can lead to a significant reduction of low-value care, whether it concerns stable angina pectoris19 or prostate cancer.20 Of course, physicians learn a lot about communication during their education and in their practice. But conversations with patients who explicitly request low-value care are challenging and require specific skills that are rarely taught in medical education. Studies show that physicians overestimate their skills for shared decision-making.21 Healthcare organisations can support the improvement of shared decision-making by promoting training, integrating decision aids into healthcare processes and ensuring that healthcare professionals have enough time to guide patients in using these tools.
Conclusion
Reducing overuse in healthcare requires more than simply identifying low-value care—it demands a fundamental cultural shift in how we perceive health, illness and medical interventions. While patient expectations and systemic incentives play a role, healthcare professionals must also acknowledge their own role in perpetuating unnecessary care and take the lead in implementing high-value alternatives. De-implementation science provides guidance for change, but true transformation hinges on continuous learning, better communication and a reframed narrative that prioritises appropriate care over providing more care. And sometimes, watchful waiting is appropriate care. By fostering a collaborative approach that includes all stakeholders, leveraging benchmarking data and integrating ethical principles into medical education, we can create a healthcare system that minimises harm by reducing overuse and maximises value for patients and society.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Footnotes
Contributors RBK and AMP discussed the issues for this editorial; RBK prepared the first and second drafts, and AMP provided feedback on both.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.