Article Text

Abstract
Background Handoffs are a weak link in the chain of clinical care of inpatients. Within-unit handoffs are increasing in frequency due to changes in duty hours. There are strong rationales for standardising the reporting of critical information between providers, and such practices have been adopted by other industries.
Objectives As part of Making Healthcare Safer IV we reviewed the evidence from the last 10 years that the use of structured handoff protocols influences patient safety outcomes within acute care hospital units.
Methods We searched four databases for systematic reviews and original research studies of any design that assessed structured handoff protocols and reported patient safety outcomes. Screening and eligibility were done in duplicate, while data extraction was done by one reviewer and checked by a second reviewer. The synthesis of results is narrative. Certainty of evidence was based on the Grading of Recommendations Assessment, Development and Evaluation framework as modified for Making Healthcare Safer IV.
Results We searched for evidence on 12 handoff tools. Two systematic reviews of Situation, Background, Assessment, Recommendation (SBAR) (including 11 and 28 original research studies; 5 and 15 were about the use in handoffs) and two newer original research studies provided low certainty evidence that the SBAR tool improves patient safety outcomes. Ten original research studies (about nine implementations) provided moderate certainty evidence that the I-PASS tool (Illness severity, Patient summary, Action list, Situation awareness, Synthesis to receiver) reduces medical errors and adverse events. No other structured handoff tool was assessed in more than one study or one setting.
Conclusion The SBAR and I-PASS structured tools for within-unit handoffs probably improve patient safety, with I-PASS having a stronger certainty of evidence. Other published tools lack sufficient evidence to draw conclusions.
PROSPERO registration number CRD42024576324.
- Hand-off
- Patient Safety
- Quality improvement
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Improving communication in the handoffs of patient care within-unit in acute care hospitals, such as that which occurs at change-of-shift, has been identified as a patient safety goal.
WHAT THIS STUDY ADDS
We found moderate certainty evidence that the I-PASS protocol and low certainty evidence that the Situation, Background, Assessment, Recommendation (SBAR) protocol improve patient safety outcomes.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Hospitals seeking to improve safety outcomes should consider using a structured protocol, either I-PASS or SBAR. Researchers should assess these and other tools in a broader set of practice contexts.
Background
The handoff (sometimes called handover) of patient care from one clinician to another has been defined as ‘a standardised method for transferring information, along with authority and responsibility, during transitions in patient care’.1 There is no single patient safety outcome metric used to assess the effectiveness of handoffs. As noted by Robertson and colleagues,2 ‘handover failures typically contribute to a cascade of failures involved in adverse outcomes, rather than being sole causes, making the estimation and investigation of handover-derived harms difficult’. Nevertheless, poor communication, including poor communication during a handoff, is one of the most common contributors to medical errors, according to The Joint Commission (TJC). TJC reports that communication failures in US hospitals were responsible at least in part for 30 percent of all malpractice claims and more than 1700 deaths over 5 years.3 Improving handoffs has been a Joint Commission National Patient Safety goal since 2006. In Sentinel Event Alert Issue 58, TJC suggests actions to mitigate patient harm caused by inadequate handoffs include standardising critical content to be communicated during the handoff and using standardised tools and methods (such as protocols, checklists or mnemonics). Handoffs and handovers are also the subject of guidance from the British Medical Association, the Royal College of Surgeons, the Australian Medical Association and the WHO.4–7 Structured protocols have been advocated to improve handoffs, the goal being to improve the communication about important aspects of a patient’s care between the clinician turning over responsibility for the patient to the clinician accepting responsibility.
Our review focuses on ‘within-unit’ handoffs rather than ‘between-unit’ handoffs. Transitions in care (eg, from the emergency room to inpatient, intensive care to general medical-surgical, post-anaesthesia recovery to general medical-surgical) have long been recognised as handoffs in need of structure and protocols and are the subject of original research studies and systematic reviews.8–15 These ‘between-unit’ handoffs have features distinct from ‘within-unit’ handoffs.16 For example, ‘between-unit’ handoffs are triggered by a change or evolution in patient illness trajectory such that the patient needs a different type of care, whereas ‘within-unit’ handoffs are regularly triggered by a change of shift. Additionally, between-unit handoffs involve an entirely new team and different modes of care, whereas within-unit handoffs are about temporal boundaries in a shift. Thus, there are conceptual differences between the two kinds of handoffs. Since there are more published reviews for between-unit handoffs, this review focuses on within-unit handoffs. Within-unit handoffs are also increasing in need and frequency due to modifications in duty-hour restrictions.17 A systematic review of structured handoff protocols to improve patient safety was considered a topic of high priority by the technical expert advising Making Healthcare Safer IV (MHS IV).
Methods
This review is based on work for MHS IV, an Agency for Healthcare Research and Quality (AHRQ)-supported review of numerous patient safety practices. The aim of this review was to assess the association of structured handoff protocols for ‘within-unit’ handoffs on patient safety outcomes. A protocol was developed for the AHRQ review and posted on the AHRQ website; additionally, it was registered with PROSPERO (CRD42024576324). AHRQ participates in setting the scope and in reviewing the final results. A multidisciplinary technical expert panel advised the project on scope. This manuscript version of the review is reported using the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) criteria.18 Data have been uploaded to the Systematic Review Data Repository managed by AHRQ and are publicly accessible. The public was not involved.
Data sources and searches
We searched PubMed, EMBASE, Patient Safety Network (PSNet) and CINAHL for the past 10 years (January 2013 to June/July 2024). Ten years was used as the look-back period in order to capture the more recent and relevant evidence. For details of the search strategy, see online supplemental file 1.
Supplemental material
Study selection
Two authors independently screened titles, abstracts and full texts. Eligibility criteria were adult and paediatric patients whose clinical care is being transferred from one clinician to another within the unit of an acute care hospital, and the intervention being evaluated was one of 12 formal tools (see below), and the study reported patient clinical safety outcomes (such as medical errors, adverse drug events, mortality). Studies of handoffs in the outpatient setting and nursing homes were excluded. Studies of handoffs between units (ED to general medical ward, intensive care unit (ICU) to general medical ward, operating room to ICU, etc) were excluded. Anaesthesia handoffs were excluded. Studies whose only reported outcome was clarity of communication were excluded. We had no study design criteria other than it had to be quantitative—qualitative studies of handoffs were excluded.
To determine what structured protocols to assess, we started with two recent review articles on healthcare handoffs.19 20 We also reviewed information from TJC3 and a list of handoff tools from Pediatrics vol 135.21 To this, we added our own search for structured handoff protocols on AHRQ’s PSNet. From these four sources, we identified these 12 structured handoff tools as appearing on the most lists or having published research on PSNet and therefore chose these as targets for this review (box 1).
List of handoff tools included in the initial search
Structured handoff tool
IMIST-AMBO (Identification/introduction, Mechanism of Injury/Medical complaint, Injuries/information related to complaint, Signs and symptoms, Treatment given/trends noted, Allergies, Medications, Background history, Other information)
I-PASS (Illness severity, Patient summary, Action list, Situational awareness, Synthesis by receiver)
ICATCH (Identify patient, Characterize situation, Action—what was done overnight, To do for the team in the morning, Confirm the handoff)
Prep 4 C’s (Preparation, Contact, Communicate, Closing the loop, Conclusion)
SBAR (Situation, Background, Assessment, Recommendation)—note there are several variants of this, such as ISBAR and SBARR
Safer Sign Out
Patient Handoff Toolkit
Targeted Solutions Tool—The Joint Commission Center for Transforming Healthcare’s targeted solution tool
PSYCH—(Patient information, Situation leading to hospitalization, Your assessment, Critical information and Hindrance to discharge)
ABC of Handover
HANDOFFS (Hospital location, Allergies/Adverse reactions, Name, DNR, Ongoing problems, Facts about this hospitalization, Follow-up on…, Scenarios)
SIGNOUT (Sick or DNR, Identifying data, General hospital course, New Events of the day, Overall health status, Upcoming possibilities with plan/rationale, Tasks to complete overnight with plan/rationale)
Data extraction and quality assessment
Data were extracted by one author-reviewer and checked by the other. Data extracted included the study design, condition, intervention type, comparison group, outcome measured and items needed to complete the Risk of Bias Tools. For systematic reviews, we used the criteria developed by the US Preventive Services Task Force that assesses reviews as good, fair or poor.22 Poor systematic reviews as determined by these criteria were excluded.22 For randomised trials, we used the Cochrane Risk of Bias Tool,23 for non-randomised studies we used the Risk of Bias in Non-randomised Studies—of Interventions (ROBINS-I) tool24 and for pre–post studies we used a modification of the NIH Tool for pre–post studies.25
Data synthesis and grading
All eligible primary studies of effectiveness were entered into an evidence table. We narratively summarised findings across systematic reviews and across primary studies. We did not conduct a meta-analysis because most of the studies were observational in design, and among the randomised trials, the settings and methods for outcome measurement were insufficiently clinically similar to support statistical pooling (eg, settings in the ICU vs the general ward; outcomes measured being total preventable adverse events vs 30-day mortality vs reintubation rate). To be included in the synthesis, a structured handoff tool needed to be assessed in more than one study or setting (ie, a single study with multiple sites of different types would be included). As these kinds of organisational changes are known to be context-dependent, if there is only one study in one context, it is impossible to assess the effect of the tool across contexts. We used the Grading of Recommendations Assessment, Development and Evaluation (GRADE) system to assess the certainty of evidence, as modified for Making Health Care Safer II26 and the National Academy of Sciences Public Health Preparedness review.27 We used single reviewer extraction with a second reviewer data checker.
Results
Our search retrieved 789 unique titles and abstracts, from which we reviewed 111 full-text articles. We found 16 articles (2 systematic reviews and 13 primary studies published in 14 publications) that met our eligibility criteria (figure 1).28–43 A listing of studies excluded during full-text review is included in online supplemental file 2. Information abstracted from each included primary study is provided in table 1.

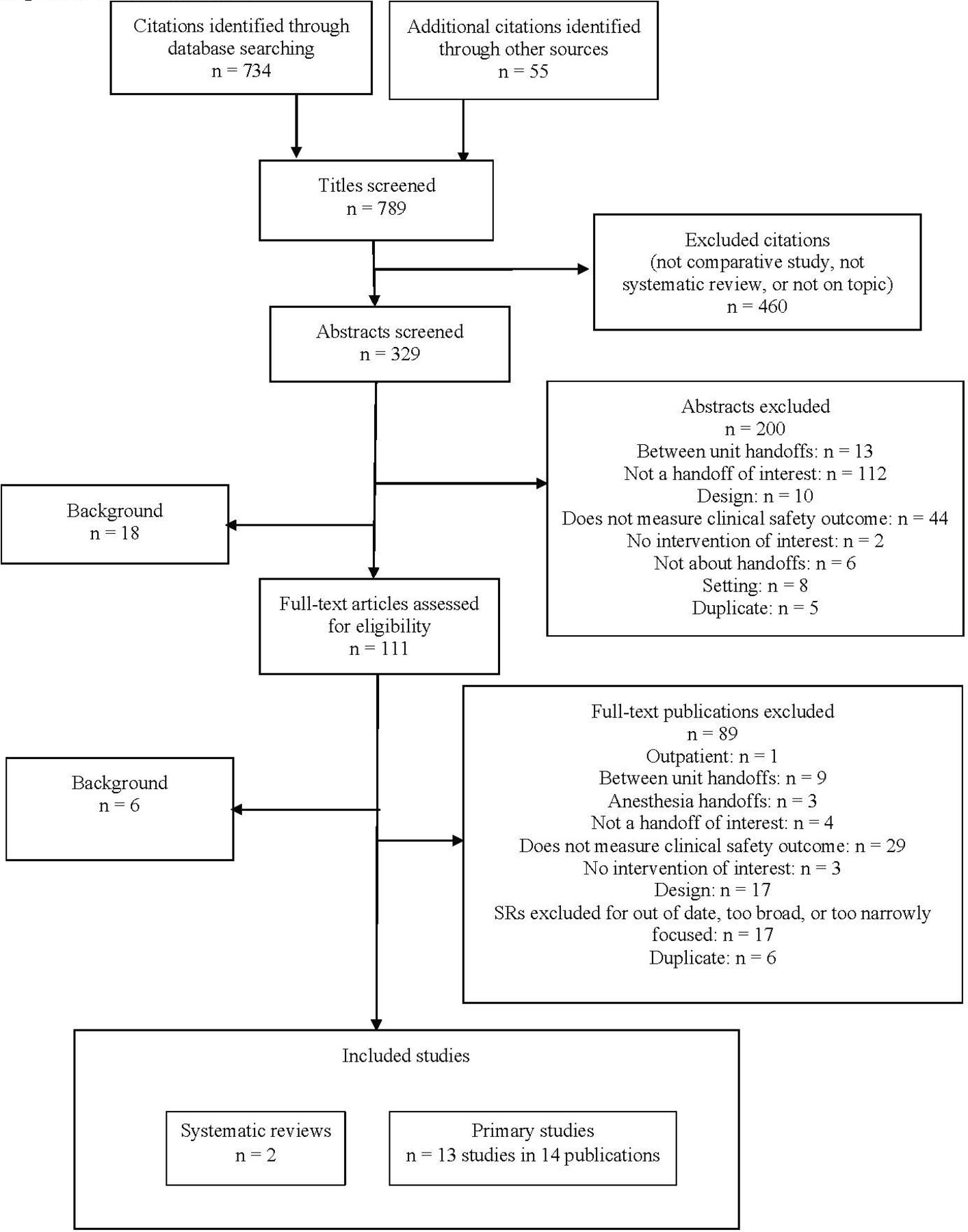{kind=link}
Literature flow. SRs, systematic reviews.
Evidence table of primary studies included
Description of the evidence
Our literature search identified 19 systematic reviews. However, seven reviews are outdated (ie, greater than 10 years from publication),2 44–49 two are more narrowly focused than our scope,13 50 eight are more broadly focused than our scope in terms of interventions or methods (such as integrative reviews)14 51–57 and/or reached inconclusive results. The two most relevant to our scope, Müller et al43 and Lo et al,42 are discussed in the section about SBAR.
We also identified 13 studies published in 14 publications.28–41 Four of the included studies were randomised trials,30 33 39 41 while the remainder were pre–post studies; two studies were performed in Argentina,29 30 one each was performed in Taiwan,40 Canada39 and Germany,41 and the rest were performed in the USA. Six studies were performed at multiple sites and the rest were single-site studies. The most commonly studied handoff tool was I-PASS, in either its original or modified form (or precursor), which was the subject of 10 studies, with 2 studies of SBAR or its derivatives,40 41 and 1 study of iHAND and SIGNOUT?.39 Most studies were conducted in academic teaching hospitals, and almost all studies assessed physician-to-physician handoffs. Most studies had numerous co-interventions/implementation strategies.
Risk of bias
Four of the included studies were randomised trials.30 33 39 41 No trial was judged to be at low risk of bias in all domains. However, the domain of blinding participants is very challenging to satisfy for this kind of intervention. Although studies are scored as high risk of bias for this domain, we did not place much weight on this assessment when considering the internal validity of the randomised trials. The remaining studies used a pre–post design. In assessing these studies, for the domain of delivering the intervention consistently across the study population, we considered any deviations to be a measure of real-world implementation and not a measure of internal validity. Thus, all studies scored well in this domain. Although the pre–post studies all scored well using the modified NIH Tool (except for two studies with very small sample sizes), our assessment of their risk of bias remains high due to the inherent limitations of the study design. The risk of bias ratings for each study are listed in online supplemental file 3.
Results for specific handoff tools
SBAR and its derivatives
We identified one good-quality systematic review about the impact of the use of SBAR for patient handoffs on patient safety.43 This review searched through January 2017 for studies focused on SBAR implementation into the clinical routine (and not a multidimensional QI intervention of which SBAR was just one component) with at least one clinical outcome reported. The systematic review identified 11 records, of which eight were pre–post studies and one study was an randomised controlled trial (RCT). Seven studies were conducted in hospitals. Nurses were the clinicians in all included studies, while in five studies additional staff were also trained in SBAR use. Five studies used SBAR specifically in handoffs, two studies used SBAR for communication in general and four studies used SBAR for nurse-to-physician telephone reporting of changes in patient status. In three of the seven studies performed in hospitals, SBAR was used only in a single unit. All studies assessed the use of SBAR by nurses, but five studies included other clinicians such as physicians. The outcomes assessed were a heterogeneous mixture of specific events like falls or patient mortality and composite outcomes such as ‘sentinel events’ or ‘adverse patient events’. The synthesis of results was narrative. The authors state ‘five of the studies found significantly improved patient safety outcomes’, ‘four other studies reported descriptive improved patient outcomes’ and concluded that there is the potential for SBAR to ‘improve telephone communication from nurse to doctors in critical situations, general patient handoff, (and) team communication in general’. Four of the five studies that used SBAR specifically in patient handoffs ‘reported an improvement of patient safety’. However, the authors noted that the quality of evidence was low, and no benefit was observed in a third of the studies.
We identified a related good-quality systematic review of SBAR.42 Although the review is not focused on clinical efficacy, we discuss it here for the purpose of continuity. The systematic review assessed the degree to which SBAR can be implemented with high fidelity. It searched through October 2020 for studies where SBAR was taught to structure verbal communication between healthcare providers or trainees, used a controlled trial design and reported any of the outcomes of fidelity to SBAR, clarity of communication, clinical outcomes or measures such as teamwork and patient safety climate. The authors identified 28 eligible studies. Most studies were conducted in hospital general or surgical wards or post-anaesthesia care units, 16 were studies where SBAR was used for handoffs, and almost 75 percent involved nurses. The studies that evaluated the fidelity of SBAR uptake primarily did so by scoring audio or video records of communication events for elements of SBAR. Ten studies reported on a heterogeneous mix of clinical outcomes such as mortality, unplanned ICU admissions, adverse events, readmissions and urinary catheter removal. As the authors state, ‘Unfortunately, none of these studies also assessed communication clarity or fidelity’. The authors found that studies of SBAR implementation reporting large improvements in fidelity all occurred in classroom settings, and studies in clinical settings reported only small-to-moderate improvements. The authors did not separately analyse fidelity outcomes by type of communication event, such as handoffs versus general communication. The authors concluded that ‘if organisations want to achieve the intended impact of SBAR, they need to attend to its implementation and ongoing monitoring’
Two new research studies of SBAR or its variants were identified. One study was a pre–post study of nurse-to-physician communication in an obstetric ward in Taiwan, although whether SBAR was being used as more of a communication tool than a handoff tool is unclear; details are in table 1.40 The other study was an RCT in Germany that assessed the SBAR variant ISBAR3 (Identification, Situation, Background, Assessment, Recommendation, Read-back, Risk)41 in seven ICU wards. The ISBAR3 checklist was delivered as an iPad mini application. Physicians received ‘brief instructions for using the tablets’ and were instructed to use the checklists as an aid during shirt-to-shift transfers which took place twice a day. Control time periods involved use of the iPad but with a different checklist—VICUR (vaccination status, insurance status, contact person, utilisation, rehabilitation)—to help minimise Hawthorne effects. During the time periods of the study, there were 1038 admissions to the ICU that met the inclusion criteria, and they were cared for by 61 physicians (61 percent of these were residents). Compared with control, there was no statistically significant difference in the three clinical outcomes: mortality, length of stay, any reuptake (readmission) to the ICU. Patients cared for during the ISBAR3 time period had worse sepsis-related organ failure assessments during the first 24 hours, but not at later time points, a finding of unclear significance. The authors concluded that ‘medical handovers are a burning issue…the present pilot study illustrates the complexity of the topic and shows both the potential and pitfalls concerning outcome parameters….’
I-PASS (illness severity, patient summary, action list, situation awareness and contingency plans, and synthesis to receiver)
We identified 10 studies about 9 implementations of I-PASS or modifications.28–34 36–38 We also include one study35 here based on SIGNOUT? as in the context of that study, it was the precursor study to I-PASS. The I-PASS Handoff Bundle as described in its landmark study37 consisted of the mnemonic, which serves as the anchoring component for all else and a number of implementation techniques and strategies. These included a 2-hour workshop (part of which was devoted to Team Strategies and Tools to Enhance Performance and Safety (TeamSTEPPS)), a 1-hour role-playing and simulation session, a computer module for use in independent learning, a faculty development programme, direct observation tools for use by faculty to provide feedback and a culture-change campaign. In the precursor study,35 the mnemonic used was SIGNOUT? (SIGNOUT? is a mnemonic for Sick or DNR?, Identifying data, General hospital course, New events of the day, Overall health status, Upcoming possibilities with a plan, Tasks to complete overnight with the plan, ? Any questions). The precursor bundle included the relocation of the handoff to a private and quiet space and the restructuring of separate house staff handoffs into a unified team handoff but did not include a faculty development programme, tools or the culture change campaign.
The precursor intervention was implemented in a pre–post study in two general paediatric wards in a paediatric residency programme teaching hospital.35 Residents are junior doctors responsible for the day-to-day care of inpatients, under the direction of a senior attending physician. The handoffs were shift-to-shift changes of physicians. The outcomes were medical errors (defined as a failure in the process of care) and adverse events (defined as preventable and non-preventable unintended consequences of care that lead to patient harm). Error reports from clinicians and formal incident reports were solicited daily. Each suspected incident was reviewed by physician investigators blinded to intervention status. Among 1255 patient admissions (almost evenly balanced between the pre-intervention and post-intervention periods), the overall medical error rate reduced from 33.8 errors per 100 admissions to 18.3 errors per 100 admissions (p<0.001). Preventable adverse events decreased from 3.3 per 100 admissions to 1.5 per 100 admissions (p=0.04). Other measures of harmful and non-harmful errors also decreased. Written handoff documentation increased markedly overall, but one unit, which used a computerised handoff tool, substantially outperformed the other unit.
The same investigators then revised their mnemonic to I-PASS, added faculty development components and a culture change campaign, and conducted a pre–post study in nine paediatric residency training programmes.37 Outcomes were medical errors and adverse events. Among 5516 pre-intervention and 5224 post-intervention admissions, medical errors reduced from 24.5 per 100 admissions pre-intervention to 18.8 per 100 admissions post-intervention (p<0.001). Preventable adverse events decreased from 4.7 per 100 admissions to 3.3 per 100 admissions (p<0.001). Other measures of harm declined, but the rate of falls, medication errors, procedure-related errors or nosocomial infections did not change. Three sites did not find statistically significant reductions in errors, and one site found more errors after implementation. Written handoff documentation greatly increased in almost all domains.
Eight additional I-PASS studies were subsequently conducted, adapting it for use in orthopaedics,38 in palliative care,29 in the ICU,30 33 to include a daily ‘rounds report’ for families,31 32 to be implemented as part of the EHR and/or in family medicine residency inpatient units,28 34 and a broader study of implementation conducted by the original I-PASS investigator.36 Not all these studies reported statistically significant effects of the intervention on clinical safety outcomes. Some studies did not use the same outcome measures as the original I-PASS study, and other clinical safety outcomes (eg, 30-day readmission, surgical site infection, reintubations within 24 hours) may not be as sensitive as the outcomes used in the original I-PASS studies. The benefits of I-PASS have not been as convincingly demonstrated in implementation studies outside the original development team.58
Other handoff tools
We identified one study on the iHAND handoff tool,39 but since it was the only study of this tool and it was a single-site study, we do not discuss it in detail here, as it is not possible to consider tool intervention effects separate from context effects. Data about the study are in the evidence table (table 1). We did not find any studies of any of the other structured tools.
Certainty of evidence
We judged the certainty of evidence that the use of I-PASS reduces medical errors and adverse events as moderate, uprated from low (based on study design) due to the use of theory/logic models, the beneficial effect of similar interventions in other areas of public safety (such as air travel), assessments of context and reporting of implementation process (see online supplemental file 3). We agreed with the systematic review on SBAR that the certainty/quality of evidence for the effect of SBAR on those same outcomes is low. No other tool had sufficient evidence to assess.
Discussion
This review found that while there are numerous structured handoff tools that have been proposed for use, there are only two tools that have been the subject of more than one study assessing their effectiveness at improving patient safety for within-unit handoffs. Those two tools are SBAR and I-PASS. Evidence about SBAR use comes predominantly from handoffs where nurses are involved (either nurse-to-nurse or nurse-to-physician). Based on the evidence from the two systematic reviews and additional new research studies of SBAR, we agree with the SR conclusions that ‘there is some evidence of the effectiveness of SBAR implementation on patient outcome’, but that implementing SBAR with fidelity is hard and that certainty/quality of evidence is low. We judged the certainty of evidence supporting the effectiveness of I-PASS as stronger than the evidence supporting SBAR, primarily due to the large, multicentre studies of the use of I-PASS. The evidence supporting the effect of I-PASS use on clinical outcomes is exclusively about physician handoffs and comes almost entirely from the developers. Implementation studies conducted in other settings and using study designs of stronger internal validity more often showed no benefits in clinical outcomes.58 However, the clinical outcomes assessed in these studies were likely much less sensitive than the medical error outcomes used in the I-PASS developers’ studies, and not all the implementation tools, such as teaching TeamSTEPPS, may have been included. That, combined with the very strong theoretical rationale for why a structured handoff tool should be effective, the repeated demonstration that the use of I-PASS increases the quality of information handed-off (data presented in some included clinical outcome studies) and the studies of implementation in numerous contexts lead to our assessment that the certainty of the evidence for use of I-PASS is moderate.
Limitations
This review is subject to the usual limitations of all such reviews: limitations in the source material and limitations of how we performed the review. The biggest limitation in the source material is the reliance on pre–post studies for most of the evidence, which increases the risk of bias. Randomised trials are few. For I-PASS, there were only two randomised trials, and neither found a statistically significant effect on patient clinical outcomes, although many of these were relatively insensitive (eg, length of stay, preventable deaths). Another limitation is that nearly all studies are conducted in academic training programmes; this could impact the generalisability of these results to non-academic settings. Evidence about SBAR is predominantly nursing, and evidence about I-PASS is exclusively about physicians. Whether or not one generalises to the other is not established. Limitations of the review process always include the possibility that we did not identify all relevant studies. Several experts reviewed our yield, but none of them identified important missing studies that met our inclusion criteria. However, this does not exclude the possibility that they may exist. We also did not re-review all of the studies included in the two reviews on SBAR; we took those reviews ‘at face value’. To re-review all the studies and reach our own conclusions was beyond our resources and negated the supposed contributions of systematic reviews to the advancement of knowledge.
In summary, handoffs are a weak link in the chain of clinical care of inpatients. Within-unit handoffs are increasing in frequency due to changes in duty hours. There are strong rationales for standardising the reporting of critical information between providers, and such practices have been adopted by other industries. Of the plethora of structured handoff tools proposed, I-PASS is the tool that has the strongest certainty of evidence in reducing medical errors and also has the most developed set of implementation strategies and tools. Future studies should focus on improving the content in handoff tools and use in other mediums such as mobile devices. Future studies should assess multisite implementation, use stronger study designs and/or methods and understand its use in other setting types (eg, non-academic settings). Lastly, this is an area ripe for studies of artificial intelligence/machine learning predictive analytics to better align the content of the handoff to the patient’s clinical context.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Footnotes
Contributors SM, AM, EL and PGS contributed equally to the manuscript. PGS is the guarantor.
Funding This project was funded under Contract No. 75Q80120D00003 Task Order 75Q80122F32009 from the Agency for Healthcare Research and Quality (AHRQ), U.S. Department of Health and Human Services (HHS).
Disclaimer Much of this work was conducted under contract 75Q80120D00003 to the Agency for Healthcare Research and Quality (AHRQ), Rockville, MD. The findings and conclusions in this manuscript are those of the authors, who are responsible for its contents; the findings and conclusions do not necessarily represent the views of AHRQ. Therefore, no statement in this manuscript should be construed as an official position of AHRQ or of the US Department of Health and Human Services.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.